Essays by
Malcolm Kendrick, MD (It’s not a plane, it’s not a train, it’s super-Celebrex-researcherman) By Red Flags Columnist, Dr. Malcolm Kendrick Studies on thousands of patients are not all the same, but they do have one thing in common. They take a damned long time. Major studies take months, or years, to set up. They then take years to do, and more months pass as the paper is written. The paper then takes several more months to go through the journal peer review system, re-writes etc. Then the results of the study get published. In mid-September 2004 Vioxx was pulled from the market for causing a high rate of heart attacks and such. In early December 2004 a study involving thousands of patients was published in the Annals of Internal Medicine clearly showing that Celebrex does not have the serious side-effects on the cardiovascular system that Vioxx has – or had. It is interesting, of course, that Merck claimed it would take years and years to do a study proving that Vioxx damaged the cardiovascular system. They also claimed it would be unethical, and probably couldn’t prove anything anyway. How little does Merck know. For a bunch of fearless researchers have managed to prove that Celebrex is two point three times as safe as the unknown risk of Vioxx in…. Well, let me see. The journal would have been going to final print in late November. The lay-out of the articles would have to be decided in mid-November at the very latest. A paper proving the safety of Celebrex on thousands of people must have taken at least two weeks, absolute minimum, to do the rounds of editor, reviewer, authors and back again. This takes us back to the end of October. It takes two weeks in an absolute tearing hurry to write up a paper (this is much faster than the fastest I have ever seen). So the authors must have started writing the paper in mid-October at the very, very, latest. Which means that this study was thought about, set-up, gained ethical approval, was carried out, and all results gathered within a month. It was then written up in two weeks, and went round the editorial peer-review process in another two weeks. I think that the Guiness book of Records should be informed. This must be the fastest clinical trial ever done in the history of the world. A record that will never, ever, be broken. Even more impressive is that, on the way, they accurately assessed the increased risk of Vioxx (something that no-one else has yet even agreed on) and managed to measure the effect of Celebrex on the cardiovascular system verses Vioxx. Not bad, not bad at all. Shame on you, Merck, for claiming such a study would have taken years. You should have employed superCelebrexresearcherman, he could have polished the whole thing off in a matter of weeks. As a sign-off, I just wonder who funded this study? JUST CALL ME THE GREAT NOSTRAKENDRICKOS By Red Flags Columnist, Dr. Malcolm Kendrick And there was a time in the past when a great wailing went up from the shareholders of Merck. For it had been revealed to them that the wondrous Vioxx didst most verily wipe out many thousands of patients with the apoplexy, and clutching at the breast, and falling down most dead. And so, the great wise men of the FDA smote Dr Graham, one of their own, and didst telleth everyone that said Dr Graham was a fool and a scoundrel and couldst not be believed when he warned of the great dangers of Vioxx. Which seemethed strange, as he was the one amongst them who stoodeth up to be counted. But we shall sweepeth this most ungracious behaviour swiftly under the carpet. With Vioxx slain, there were those, the great Nostrakendrickos foremost amongst them, who gazed into the future, and he had a most powerful and disturbing vision. He saw another drug, the drug called Celebrex. In his vision it was standing strong and proud amongst the desolation that had been Vioxx sales. It seemed immensely powerful, impregnable, a massive fortress bringing vast profit and wealth to those who had Pfizer shares. But Nostrakendrickos was most disturbed by the sight of a huge vulture in the skies above the Celebrex fortress. This, he felt, foretold doom. For the vulture, surely, was the same one that had been circling Vioxx shortly before. A great battle ensured, with bolts of lightening being hurled into the sky by the plucky marketers defending Celebrex. They hoped to blind everyone to the facts, including the vulture. But Death’s head slowly emerged into the vision, undeterred by such tactics. And from its gaping rotten maw a voice could be heard. ‘This is a class effect…..this is a class effect.’ The voice of Death brought anguish and fear to the hearts of all who heard it. Particularly those in the legal department of Pfizer. They ran screaming to their huge condominiums, and huddled in their Jacuzzis, hoping to be spared the terrible lacerating court cases. The vision faded and Nostrakendrickos was jolted back into this World, the sights he had seen still etched into his memory. Lo, he predicted, Celebrex would do most well to survive the Winter Equinox. And most surely it came to pass that a study didst emerge demonstrating that Celebrex too dids’t cause the apoplexy and the clutching at the breast and the falling down most dead. Actually, it didn’t quite happen like that. But it makes for a much better story don’t you think. In reality it was just a matter of time before the truth about Celebrex emerged, and now it has. Interesting to see how Pfizer decide to jump. My bet is a reluctant withdrawal, but I would love to be a fly on the wall as the decision is debated. Oooh, the sound of heads rolling. Merry Xmas to everyone marketing Celebrex. (I know it’s happy holidays over there, but we’re still allowed to say Xmas in the UK – just)
AN ASTONISHING FINDING THAT FAILS TO SURPRISE By Red Flags Columnist, Dr. Malcolm Kendrick Baltimore, MD - Researchers have found that 100% of industry-sponsored studies recently presented at the annual scientific meeting of a medical professional society reported findings that support product use. The study, by Drs Thomas Finucane and Chad Boult (Johns Hopkins School of Medicine, Baltimore, MD), appears in the December 1, 2004 American Journal of Medicine. Well, well, blow me over with a feather. Quelle surprisé. Who would have believed it? Well I never. And other phrases that don’t exactly spring to mind. So, comrades, every single paper presented at a scientific meeting, funded by a pharmaceutical company, supports the use of their products. I mean, even ruthless dictators running their countries with a rod of iron never manage to gain more than about 99.87% of the popular vote. I always wonder what happens to that 0.13% of voters, or thereabouts, who do not vote for the only candidate on the voting paper. But pharmaceutical companies, apparently, can do better than any dictator when it comes to a vote of confidence. They can carry out trials which are one hundred per-cent positive. Never a doubt creeps in, not one. And, to quote the authors on the matter of positive trial presentation at meetings. ‘I would be astonished if this were true of only one medical society.’ Hey guys, so would I. Does it matter, does anyone believe anything that comes out of these studies. Aren’t all doctors capable of spotting bias? To quote the authors again. ‘With compelling evidence that the knowledge base produced by commercially sponsored research is biased, with evidence that physicians do not reliably detect bias in information presented to them, with no evidence that bias in individual studies is reliably detected and discounted, and with repeated examples of manufacturers using potentially biased evidence largely to promote sales…what commercially supported research can be trusted?’ A good question my friends, a good question indeed. Frankly, if I wanted to be believable, I would slip in the odd negative study from time to time, just to keep people thinking that I was upright and honest. The problem with reaching the magical one hundred per cent figure is that it always just seems too good to be true. And where do you go from here. ‘Guys, we have achieved a one hundred per-cent positive publications record on one our drugs, but now we want more. We want one hundred and ten per-cent.’
But I have some sympathy. The pressures on the marketing people in pharmaceutical companies is becoming ever more intense. They are virtually forced to accentuate the positive, maybe even distort the facts a little, bribe (sorry did I say bribe, I meant ‘pay honoraria to’) a few senior doctors here and there. Anyone who stepped out of line within a company, and tried to present all the data, good or bad, would rapidly find themselves heading for the unemployment office with a large boot applied to their posteriors. Those whose ethics start to trouble them too much just leave. Others have mortgages to pay, best to keep your head down and keep quiet. For now, the media doesn’t yet dare to attack the medics who promote this type of work, they fear being shredded by a clever specialist. Who dares take on the expert in their field of expertise? Which means that medical journalists are still happy to regurgitate the distilled messages created by PR firms and fed into the mouths of international experts. And the public still trusts the senior docs - just. But I suspect that the elastic band of trust has now been stretched to the point where it just needs a couple more tweaks before it snaps back painfully. You can only distort the data so far before everyone finally wakes up and takes notice. ‘You can fool all of the people some of the time and….’ You know the rest. We are, I think, very close to the breaking point, and the situation has now become dangerous and potentially damaging. To quote again ‘Drug companies corrupt science in a way that is directly harmful to patients.’ Their words, not mine. I wish it were not true. Drug companies could be a force for good, they have the potential to be a part of the solution to improving health care, and I think that they have generally been a force for good. However, through the inexorable drive for more sales to feed the little fledgling shareholders, mouths agape, drug companies have now become part of the problem. For now, if you see headlines proclaiming ‘Drug x found to reduce deaths by thirty per-cent,’ or whatever, it would be safer to ignore the finding. The only ones that you should believe are ‘Drug X found to cause sixty zillion deaths.’
More essays by Malcolm Kendrick
GROUNDHOG DAY – IN REVERSE By Red Flags Columnist, Dr. Malcolm Kendrick Imagine waking up and having no recollection of anything that happened the day before. All memory, wiped, gone. You find a letter written by yourself that you can’t remember writing. You go out to buy a present only to find, when you get home, that you had already bought it. Your next-door neighbour asks for his wheelbarrow back, the one he lent you yesterday, you look at him blankly and say you haven’t got it. You would think you had gone nuts. The foundations of your existence severely shaken. What the hell has happened to me? Have I had a stroke, am I very ill, did someone spike my drink? None of the above. What you may have been doing is taking a statin. For some time now I have been in contact with a US doctor, who trained as an astronaut, no less. I am most jealous. Even if he has never gone into space he must have got to see the space programme at close range. I am a sucker for space exploration – the final frontier and all that. Anyway, he had been taking Lipitor (atorvastatin) when, one day, he completely lost his memory for a few hours. This was a horribly disorientating experience, and caused him to think all sorts of frightening thoughts. Brain tumor, stroke, the usual sort of medical fears we all have in the wee small hours. He didn’t think that this could have anything to do with the statin, as he had never heard of this side effect, nor read about it. However, he came off the Lipitor anyway. But when he went back on, same thing happened. He asked his own doctor if the drug could cause the problem and was assured that this was not possible. He wrote to Pfizer, who said they had never heard of such a thing – adding that safety is their number one priority, no doubt. He could find no-one who would support his guess that atorvastatin was the cause of his amnesia. But he did take some further action, and put out a few messages on the internet asking if anyone else taking a statin had experience the same problem. Within a short space of time he had received hundreds of replies from people who had experienced exactly the same thing. Still the medical establishment ignored him, as did Pfizer. He then started to find out a bit more about statins drugs, and cholesterol, and the whole lipid lowering industry. He came to realise, for the first time, that almost everything he believed about heart disease and diet, and cholesterol, and cholesterol lowering was total bunk. Ah, joy, another convert. He also discovered that cholesterol is absolutely and totally essential for the creation of new synapses in our brains. Mainly because new synapses in our brains are made almost entirely from cholesterol. So it did not seem biologically impossible that, if you take a drug specifically designed to block cholesterol synthesis throughout the body (There are cells in our brains that manufacture cholesterol, it is not just made in the liver), you could prevent the formation of new nerve cell connections – and thus memories. The need for cholesterol to make nervous tissue function properly is highlighted by the fact that if you take a statin in the first trimester of pregnancy, development of the nervous system in the unborn child can be horribly deformed. Yet no doctors anywhere, apart from him and me, and a few other ‘cranks,’ are willing to accept that statins could cause transient global amnesia (TGA). So, if you are on a statin, and you do suffer from TGA this will not, ever, be recorded as an adverse effect of the drug. So the FDA has no record of it, and the statin manufacturers can place their hands over their hearts and declare that there is no evidence at all that statins can cause amnesia. Because no-one has ever reported it (see under Vioxx). Somewhat frustrated – I know the feeling Duane – he wrote a book about his experiences, and thoughts, and research, on the whole damned idiotic cholesterol lowering world of madmen. It is called LIPITOR, THIEF OF MEMORY (statin drugs and the misguided war on cholesterol) by Duane Graveline MD MPH is now available from www.spacedoc.net or www.buybooksontheweb.com Please buy it, read it, and stop taking the statins. If, of course, you can remember whether or not you are taking them in the first place. Also, please ask your airline pilot, yelling through the reinforced security door, if he (or she) is taking a statin. An episode of TGA whilst piloting a plane could be a most interesting experience for everyone involved. ‘Gee, what the hell are all these knobs and dials for anyway?’ (Exit to sound of plane plummeting into the ground)
More essays by Malcolm Kendrick
A SUGARY TALE (First article in a series on ‘type II diabetes’) By Red Flags Columnist, Dr. Malcolm Kendrick For the last thirty years, give or take, people with type II diabetes have been instructed to eat a low fat high carbohydrate diet. Why? Because it is ‘known’ that a high fat diet causes heart disease. It is also known that people with type II diabetes have a greatly increased chance of dying of heart disease (true). Ergo, type II diabetics should not eat fat. And so, most people with type II diabetes now slavishly follow a diet that is, in all likelihood, doing them considerable damage, based on a misguided belief that fat in the diet is harmful. In reality, the last thing that someone with type II diabetes should do is eat a high carbohydrate diet. I know that, for most people, this sounds utterly counter-intuitive. But I would like to take you on a journey into the world of type II diabetes, one that I have travelled over the last two years. It’s a bit of a winding path, primarily because a lot of misinformation needs to be unwound before it is possible to re-start with a clear slate. I hope that, at the end of this journey, you will understand what type II diabetes actually is. In truth, I hope you will understand that there is no such disease as type II diabetes, that there is no such thing as insulin resistance, and that almost everything you think you know about this area is, not so much wrong, as tangled up in a big mess. The start I became interested in type II diabetes as a result of my fascination with heart disease. I knew that there was a strong connection between the two, and so I realised that I had better find out more about type II diabetes. What it was exactly, what caused it, that sort of thing. At first sight the disease process itself seemed very simple. As you get fatter, the body, in an attempt to fight back, becomes more resistant to the effects of insulin. At one level this makes sense. The main function of insulin is to switch on various food storage mechanisms in the body, so if you can block these actions you can, presumably, fight against weight gain. The downside, of course, is that sugar levels go up, as sugar is trapped in the blood. Like many others I nodded sagely when resistin - a direct antagonist to insulin released by fat cells – was discovered. It seemed that a simple negative feedback loop was in operation with the body battling against excess food storage through ‘insulin resistance.’ By golly, it all made sense. Then, one day, I thought about it a bit more, and started mentally picking at something that looked like a small flaw, a loop in the jumper if you like. After a bit more picking the entire jumper suddenly fell apart in my hands, and I realised that what had looked like a fine upper body garment was, in fact, just a set of disconnected loops made to look like a jumper. As I gazed at the metaphorical unravelled ball of wool lying at my metaphorical feet, I knew that the simple model linking obesity to insulin resistance and type II diabetes made no sense at all. So I had to gather up my thinking and start again, from the beginning – which is a very good place to start. And I began by looking more deeply into obesity, and what effects it should have on insulin release and insulin sensitivity. At its most simple level obesity can be thought of in the following way. If energy input is greater than energy output you will put on weight. Therefore, to lose weight you can reduce input, or increase output. Which may seem like a statement of the obvious. What may be less obvious is that insulin has absolutely no effect on either of these things. Insulin does not (except perhaps in the most minor fashion) reduce hunger, or block food absorption. Nor does it increase the metabolic rate. Nor does it stimulate you to go out and take exercise. Nor can it force the body to excrete energy - the body has no system for excreting energy anyway. Therefore, if you become resistant to the effects of insulin, and levels rise, what exactly happens to prevent weight gain? Nothing much would seem to be the answer. All of the food you eat will still be absorbed, and once absorbed it has to be stored somewhere. At this point it is probably worth running through the energy storage systems in the body, before returning to the main argument. There are, basically, three forms of stored energy, and three places they can be stored. Energy can be stored as
Energy can be stored in:
And that’s it. There are no other forms of energy (of any significance), and nowhere else to store it. If, as you get fatter, muscle, liver and adipose tissue become resistant to the effects of insulin, where does the excess energy go? Well, as you have probably worked out, there is nowhere else for it to go but adipose tissue. You can’t squeeze more energy into the muscles or the liver, they can’t take it (not quite true, you can end up with a fatty liver, but this still represents a minute amount of the total energy store). The brain kidneys and lungs cannot store energy. It doesn’t go into bones, and it certainly can’t disappear into thin air. Thus, whilst insulin resistance does make it more difficult (if that’s the right word) to store excess energy as fat, it will still happen anyway, because there is no alternative. So what, exactly, is the point of that? As I hope is now obvious, once you start thinking about it, it becomes clear that insulin resistance can do nothing to prevent obesity (this was my loop in the jumper). Which means that insulin resistance does not represent an adaptation, or negative feedback loop, designed to prevent obesity. Or, if it is, then it is the most stupid feedback loop discovered. Because it can’t work. In short, there is no way that obesity, or a raised BMI, can be linked in any simple fashion to type II diabetes. Yet, and yet, when you study this area there seems little doubt that an increasing BMI does appear to be the most important risk factor for developing insulin resistant diabetes – type II diabetes. For example, women with a BMI of more than thirty five have a ninety times increased risk of developing type II diabetes, versus women with a BMI less than twenty five. On the other hand, if you have a BMI of about twenty two (slim), you have almost no chance of developing type II diabetes. If these were the only pieces of data that you had, then it would seem reasonable to suggest that obesity is the cause of type II diabetes. However, there are plenty of other data that don’t fit so neatly, if at all. However, by the time these bits of data emerged the mainstream had made its mind up. Obesity causes diabetes. And so, rather than open up the area for another look, all contradictory data has been made to fit, which has created a confused mess. So, what is the contradictory data, exactly. The first problem, which is not exactly contradictory, is that most obese people do not suffer from diabetes. Which suggests that obesity is not sufficient to cause diabetes. We do not have a simple causal relationship. You may not think that this is a huge problem, some people are just more susceptible than others – hold that thought. A much more fundamental problem is that you can find non-obese populations who have high rates of insulin resistance. Emigrant Asian Indians, for example, have a frighteningly high rate of type II diabetes although they are much less obese, on average, than the surrounding Caucasian populations. This is also true for emigrant Japanese in Brazil and the USA, Australian Aboriginals, and Native Americans – and others too numerous to mention. So, although it is true that obese people are much more likely to get type II diabetes than thin people. It is also true that most obese people do not have type II diabetes, and you can also find several non-obese populations suffering from very high rates of type II diabetes. Which means that obesity is neither sufficient, nor even necessary, for type II diabetes to develop. And, if you keep looking, the association between obesity and diabetes fragments even further. For example, if you remove more than twenty five pounds of fat through liposuction this has no impact whatsoever on sugar levels/insulin resistance. On the other hand if you lose twenty five pounds on a diet, this will almost completely reverse insulin resistance (at least temporarily). Um? And looking at the Japanese again, we find that Sumo wrestlers – who have BMIs that put them in the super-obese category – have no signs of insulin resistance at all. I could go on, but that’s enough contradictions for now. So how would you go about fitting all of these facts together? In general, when you find direct contradictions to your central hypothesis you have two choices. Choice one is to develop an ad-hoc hypothesis to explain each contradiction. Choice two is to rip up the model and start again. The mainstream research community decided to go down the ad-hoc hypothesis route. For example. Question: Why do emigrant Asian Indians have such a high rate of type II diabetes (up to 60% in some studies), despite having much lower BMIs than Caucasians. Answer: They are genetically susceptible to developing type II diabetes; therefore we need to re-define obesity in this population. Let’s lower the ‘obese’ BMI to twenty five instead of thirty. (In this way, they fit back into the hypothesis) Genetics always provides a good catch all explanation for almost any contradiction. If you find an obese group with low rates of type II diabetes they are ‘genetically protected’, if you find a group with high rates of type II diabetes despite being non-obese they are ‘genetically susceptible’. Ergo, when you find that Australian Aboriginals have an even higher rate of type II diabetes, with an even lower average BMI than Emigrant Asian Indians, you can lower the BMI that defines obesity in this population to around twenty two (which has happened). This is known as stretching the hypothesis to fit the facts. By constantly redefining obesity, you can still claim that obesity is the underlying cause of type II diabetes in all populations. (You may recognise this ‘altering the boundaries of normal’ technique from the Cholesterol hypothesis. Keep lowering the level considered raised until everyone has a raised level). Oh yes, genes are most wonderful things. They can explain away contradiction after contradiction (so long as you don’t think about it too hard). It’s like playing a joker in a game of cards; you can never lose when you invoke genetics. Apart from genetics, there are many other ad-hoc hypotheses that are thrown into this particular mix to explain away other contradictions. However, rather than going through them all, one by one, I chose the opposite approach. I decided to rip the central hypothesis up and start again. See if I could find another, better, hypothesis. One where the facts all fit snugly into the hypothesis, rather than the other way round. This is always my preferred route. But in order to travel down this route you have to question everything, even the things that seem written in stone. Here are four, almost sacrilegious, questions that I asked myself. Question one:
does obesity cause diabetes? And you know what, after doing this, everything started to fall into place. Although I had to spend several months learning a great deal more about human physiology and energy metabolism.
More essays by Malcolm Kendrick
BERARDINELLI-SEIP – EXPLAIN THAT? By RFD Columnist, Dr. Malcolm Kendrick For those of you who read my last article, ‘A sugary tale’, and who didn’t agree with a word that I said, which could well be almost everybody. I would like to introduce you to a fact that you may find surprising – to say the least. Just to rewind for a moment. Basically I said that obesity probably wasn’t the underlying cause of type II diabetes. (I also said that there was no such disease as type II diabetes, but we’ll get to that later). In order to prove my first point I thought it would be interesting to try and find out if there is a population with zero adipose tissue to see what happens to their insulin resistance, levels of blood sugar, and rate of type II diabetes. If such a population exists do you think they would have a high rate of type II diabetes, or a low rate? At this point you are allowed to have a guess. It has to be said that there are not many people on the planet who have no adipose tissue at all. My first port of call was to look for information on body builders, who make strenuous efforts to reduce their body fat almost to zero. I already knew that they had somewhat disturbed metabolisms, with a propensity to early heart disease. However, these people eat such strange diets and take such strange drugs and supplements that I thought it was best to steer clear on the basis that anything I did find was likely to be almost impossible to interpret. What I needed to find, if possible, was a population with no adipose tissue at all. I didn’t hold out any great hopes that such a population exists, but much to my surprise, it does. There is a very small group of people out there who suffer from a rare condition known as Berardinelli-Seip syndrome, first described by a Mr Berardinelli and a Mr Seip. This is a genetic disorder of ‘lipodystrophy’. Lipodystophy means a total or partial loss of body fat. In the case of Berardinelli-Seip there is a total loss of body fat. No body fat, no obesity, therefore no diabetes…. right? Ah, wrong. Every single person with this rare syndrome develops type II diabetes. I shall let that sink in for a moment.
So, you still think obesity causes diabetes? If so, please let me know how you explain Berardinelli-Seip Syndrome. By the way, their only abnormality is a complete lack of adipose tissue, in all other ways they are normal (just in case you were wondering). Before you get too confused, I shall present the mechanisms leading to type II diabetes in BS syndrome (you don’t think I’m going to keep typing out Berardinelli-Seip syndrome do you) In BS syndrome you have no adipose tissue. Therefore, if you eat more than you need, where can the body put this excess energy? There are only three possible places. Muscles, liver and blood. However, the muscles and liver can only store about four to five thousand excess calories as fat and glucose/glycogen, max. So doesn’t take long to overload the total energy storage system, resulting in raised blood levels – of almost everything. Which means that, in BS syndrome, you can pump the insulin levels up as high as you want, but the muscles and liver cannot respond by increasing their storage capacity. (Obviously muscle can store protein as muscle, but this is not really an energy store). Once they are full, they are full. And there is another problem in BS syndrome, which compounds the vastly reduced food storage capacity. This is the lack of the hormone called leptin. Fat cells all produce leptin which, at a certain blood level, tells the brain that there are sufficient fat stores. When the total fat stores drop below a certain point, little leptin is released, and the brain gets the message ‘Eat!’ With no fat stores at all, those with BS syndrome are often ravenously hungry – all the time. Which adds greatly to their problem. They are stuffed full of energy, yet their hormonal system is driving them to consume food. So, in BS syndrome you are constantly hungry, yet there is no adipose tissue to store the excess energy you consume. What, then, would you expect to see happen.
In BS syndrome muscles are oedematous, full of glucose and thus water. Each glucose molecule is surrounded by sixteen water molecules – it’s a chemical thing. So if you fill muscles beyond their normal glucose capacity, they will also, effectively, fill up with water. The liver is also ‘fatty’ in BS syndrome. Normally, the liver gets rid of excess glucose by turning it into triglycerides and exporting it to adipose tissue. However, in BS syndrome there is no adipose tissue, so fat ends up trapped in the liver
As stated above, when confronted with excess glucose, the liver turns this into triglycerides, packs these triglycerides into Very Low Density Lipoproteins, and exports them to adipose tissue. However, in BS syndrome there is no adipose tissue, so the VLDL level skyrockets. The thing that amazes me about BS syndrome is that it is possible to live for more then a few months before the entire metabolism just explodes under the strain. Yet sufferers can live for many years, and they are now being ‘treated’ with leptin to stop them from feeling hungry all the time and eating too much food. Apart from looking very gaunt they seem healthy enough. The thing that does not amaze me about BS syndrome is that it leads to ‘type II diabetes.’ Or at least the spectrum of metabolic abnormalities that we call type II diabetes. How could it possibly be otherwise? Yet, when it was first discovered that those with BS syndrome all had type II diabetes everyone was, apparently, astonished. Why were they astonished? Because all the experts know that obesity causes type II diabetes, yet here were a group of diabetics without a single adipose cell, so how could they develop type II diabetes? The answer to this apparent conundrum is very simple, but it requires that you start looking at things from a completely different perspective. Those with BS syndrome do not develop type II diabetes, because type II diabetes is not a disease. It is just a set of metabolic abnormalities – primarily a raised blood sugar level. The ‘disease,’ if there is one, is whatever causes the blood sugar level to be high in the first place. And there are several things that can do that. The most clear cut examples are:
Treat these conditions, or diseases, and the blood sugar level drops. Have we ‘cured’ type II diabetes? No, we have just lowered the blood sugar level. Until people can rid their minds of the pernicious concept that a raised blood sugar level is a disease, and that lowering it represents disease treatment, it is almost impossible to have a discussion in this area. At the risk of repeating myself I will restate that nothing, and I mean nothing, confuses things more than the idea that a measurement (a raised blood sugar level), is a disease, and that by lowering this measurement (a raised blood sugar level), the disease is treated/cured. A measurement is not a disease, and vice-versa. Thus, the answer to the first part of the BS syndrome ‘paradox’ is simple. Stop calling a raised blood sugar level a disease and the problem disappears. Remain stuck with the thought ‘paradigm’ that a raised blood sugar level = diabetes, and you will never be able to understand anything in this area. Moving on, even if you don’t call a raised blood sugar level type II diabetes, how can you explain why people with a lot of adipose tissue often seem to develop the same metabolic problems as people with no adipose tissue. And if you want to know the answer to this, read on. And if all I have done is to make your brain ache, then you should also read on. Because from this point on, I shall start making things simple again and the brain ache should settle down – maybe. More essays by Malcolm Kendrick
CONFLICT OF INTEREST – TIME TO COUNT THE SPOONS? Some Thoughts After Discovering That Some Members Of A Panel Recommending New Statin Guidelines Had Big Pharma Ties By RFD
Columnist Dr. Malcolm Kendrick
As P.G. Wodehouse once wrote (sic) ‘When an Englishman says ‘trust me’ it’s time to start counting the spoons.’ At what point does the same hold true for an international medical opinion leader? A few years back the Attorney General in the United Kingdom, Lord Irvine, ( Britain's highest ranking legal figure), was accused of acting in an improper fashion. He had asked various barristers for donations to the Labour Party – which was in power at the time – and Lord Irvine was both a member of the Labour party and personal friend of Tony Blair. As he also got to choose who was going to become a Judge, next step up from Barrister (or next step down, if you share my opinion of the legal profession), it was felt that he could, just possibly, be seen to be applying pressure on innocent young lawyers and abusing his position. However, as Attorney General, he was in a position (for complex legal and constitutional reasons) that meant he was above investigation. So Lord Irvine, instead, chose to scrutinise his own behaviour. After carrying out an exacting examination of himself he reported his findings. I cannot remember his precise words, but they went something more or less like this. ‘I have looked at my behaviour in great detail. Despite an exhaustive and robust enquiry I can find nothing wrong with what I have done. As I know myself better than anyone else I believe that I was in the best position to carry out this review, and I am fully convinced that my behaviour met the highest ethical standards. I trust this will be the last that I hear of this matter from myself.’ Okay, I exaggerate for effect, but not much. At the time many commentators were left gasping by the sheer arrogance of the man. I think my own response was the highly eloquent..but…but…but…I mean..what. As Robbie Burns, a great Scottish poet (for those who don’t know), once said. "Oh wad some power the giftie gie us, to see oursels as ithers see us.” Obviousl y, he wasn’t very good at spelling. It is always a problem when we decide to investigate ourselves, or our peers. Firstly, no-one ever believes it when the investigation clears the alleged wrong-doer. For many years in the UK the police used to investigate allegations against other policemen. From a credibility stand point this was a disaster. It’s like filling a jury with CEOs to decide on the guilt of the Enron Board. Any chance of a not guilty finding? And the greatest problem with medical opinion leaders is that there is no external system to judge their behaviour. They aren’t appointed by anyone, and there is no ‘International Opinion Leader Council’, no standards of behaviour, no ethical committee. It is, to use a UK term, the ultimate ‘old boys network,’ where the most important consideration for membership is the question ‘but is he a good chap?’ I am certain that all of these opinion leaders believe themselves, just like Lord Irvine, to be acting from the highest moral principles. They are, after all, eminent in their field. How could we, the lesser beings, even dream of suspecting that their views may, just may, be biased by the payment of large sums of money. Do we not realise that these people are singularly capable of clear sighted and robust self-assessment. None of them, it would appear, ever accepts the possibility that they could be nudged from the pathway of pure objective scientific research by financial considerations. And do they not know themselves better than anyone else ever could? You never know. It could even be true. After all as National Heart, Blood and Lung Institute (NHBLI) - part of the NIH - said in a recent press release. ‘ The members of expert panels charged with developing guidelines are selected for their scientific and medical expertise, their stature and track record in the field, and their integrity.’ This response came after the NHBLI was stung into action by widespread criticism that the close financial ties between those developing the guidelines, and the pharmaceutical industry, had not been revealed. I am interested in the claim that the members of the panel they were selected on their integrity? What selection criteria were used to validate integrity? Did one of them own up to breaking wind in a lift? Which one chopped down the cherry tree? Or could it possibly be the case that no-one has the slightest idea of the integrity of the members of the expert panel. I know where I’d put my money. To paraphrase the great P.G. Wodehouse ‘When an international medical opinion leader says ‘I have great integrity,’ it’s time to start counting the spoons.’ More essays by Malcolm Kendrick
Cholesterol And The French Paradox, The Swiss Paradox, The Russian Paradox, The Lithuanian Paradox...Etc... By Red Flags Columnist, Dr. Malcolm Kendrick I was going to write about something else, but I couldn’t resist bringing the latest results from the MONICA study to your attention (MONItor trends in CArdiovascular disease). This study has been going on for ages now. It was set up by the WHO – not the rock band - to look at heart disease rates and risk factors in twenty six countries across the world. MONICA is a fantastic study by the way. It creates huge volumes of data which can be relied upon to be accurate and objective. Three cheers for the WHO for having the foresight to put this study in place. Talkin’ bout my generation. For years the MONICA study can remain silent then, every so often, it bestirs itself and out plops a golden egg. The latest golden egg comes from their review of high cholesterol levels in countries ranging from China to Northern Ireland. They decided to find out what percentage of the male population in nineteen of the MONICA countries (don’t ask me why they chose nineteen), had a cholesterol level greater than 6.5mmol/l ( 260mg/dl.). This is a fairly good indicator of the average cholesterol level in a country. The figures ranged from a prevalence of about 2% in China, to 51% in Switzerland. In short, MONICA revealed a twenty five fold difference in the prevalence of high cholesterol between countries, which was the somewhat unimaginative headline attached to the study. ‘Prevalence of high cholesterol varies 25-fold.’ Actually, it varies 25.5 fold. However, what I found far more interesting than this bald statistic was the fact that there appeared to be absolutely no relationship between the percentage of men with high cholesterol levels, and the rate of heart disease in those countries (with the possible exception of China). A fact that appears to have passed without comment. Least said soonest mended? For example, the rate of CHD in Russia is enormously high, yet the prevalence of high cholesterol levels in Russia was third lowest. On the other hand the rate of CHD in France is very low, yet the prevalence of high cholesterol levels in France was in the top half of the table. In order to confirm my suspicions about the lack of association I made a rapid search of my archives in order to establish CHD rates in the nineteen countries chosen by MONICA. Then I matched them to the percentage of men in each country with high cholesterol levels. I used the latest full year where data is available for CHD rates in each of the nineteen countries (1990) – unfortunately, one of the countries was Yugoslavia, which doesn’t exist any more, then plotted this against hypercholesterolaemia rates, from MONICA, five years later (not perfect but then cholesterol levels haven’t changed that much over five years). This resulted in the graph you can see below.
Each of the points on the graph represents a country. Bottom left is China, with a CHD rate of ‘sixty per hundred thousand per year’, and a raised cholesterol level prevalence of two per cent. The highest point is Lithuania; with a CHD rate of five hundred and eight five and a raised cholesterol level prevalence of just over thirty per cent. Far right is Switzerland, CHD rate one hundred and eighty one, raised cholesterol prevalence fifty one per cent. I have no doubt that a statistician could apply an elegant mathematical formula to that graph, and end up with a straight line leading from bottom left to top right ‘proving’ that the percentage of the population with hypercholesterolaemia is strongly and consistently related to the level of CHD. I am sure that super-computers around the world are humming away madly as they attempt to find the statistical equation that matches the approved ‘answer.’ For myself, all I can see is a French ‘paradox’ and Swiss ‘paradox’ a Russian ‘paradox’ a Lithuanian ‘paradox….. My interpretation is that there is absolutely no connection between cholesterol levels and CHD rates in these nineteen different countries. Once again MONICA comes up trumps. In fact MONICA has been producing results directly contradictory to the cholesterol hypothesis for years;it’s just that somehow or other the results always get smoothed over. In this case, however, I would have to take my hat-off to anyone who is capable of smoothing that particular graph. They shall be crowned medical statistician of the decade. (Which is not actually a compliment in my book). More essays by Malcolm Kendrick
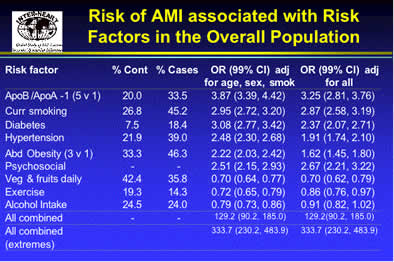
Sneak Attack! A Major Shift In Heart Disease Risk Assessment Has Whipped By Right Under Our Noses In A New Global Study...Say Goodbye To Raised Cholesterol/LDL As A Risk Factor In Heart Disease By Red Flags Columnist, Dr. Malcolm Kendrick (email - malcolm@llp.org.uk) Inspector Gregory: "Is there any other point to which you would wish to draw my attention?" Holmes: "To the curious incident of the dog in the night-time." Inspector Gregory: "The dog did nothing in the night-time." Sherlock Holmes: "That was the curious incident," remarked Sherlock Holmes. From "The Adventure of Silver Blaze" by Arthur Conan Doyle It is always a great deal easier to see the things that are there, than the things that are not. But sometimes that which is missing is far more important. Far, far, more important. I remember, years ago, being shown an x-ray of a child’s leg. I was asked what I could see. I looked and looked, but I couldn’t see a damn thing wrong. After a couple of minutes of head scratching it was pointed out that there was no fibula. A very rare congenital abnormality, leaving only one bone in the lower leg instead of two. I, who was looking for the presence of something, completely failed to notice the absence of a thing. I am sure that magicians use techniques like this all the time. You are looking for the trick, but the trick already happened and it was something the magician didn’t do, rather than what he did. I was reminded of my absent fibula – an incident that still brings a small flush of embarrassment, even now – when I started reading about the INTERHEART study, the results of which were recently presented at the European Society of Cardiology conference in Munich. This was a massive study involving tens of thousand of patients, and more than two hundred centers around the world from Asia to Africa to the US. It was designed to establish, for good and all, what really and truly are the major factors that cause, or prevent, heart disease worldwide. I thought I should reproduce a slide from the presentation on INTERHEART. It is rather busy, but it has the advantage of being straight from the horse’s mouth – so to speak.
Many of the usual factors are there. Smoking, diabetes, high blood pressure, abdominal obesity. These are the bad factors. Alongside this are the protective factors which include exercise, drinking alcohol and eating fruit and vegetables. Of particular interest to me, is the impact of psychosocial ‘stress.’ However, what is most intriguing is the deafening noise of a dog failing to bark. If you close your eyes and listen closely you may be able to not hear it. Have you noticed it yet? If not, let me draw your attention to the ‘the curious incident of the cholesterol level that did nothing’. Study that slide again and ask yourself. Where is cholesterol and/or LDL level? Surely a raised LDL level is THE most important and powerful risk factor for CHD? We have been told this enough times. Yet, it barketh noteth. In fact it is completely silent. Apparently, it has no impact at all on the risk of CHD across the World. None. Instead we have the ApoB/apoA-1 ratio. Which, it is true, has something to do with lipoproteins and cholesterol. But it has nothing directly to do with the cholesterol/LDL level. Nothing. Now, I am not a gambling man. But I have been granted the ability to see into the future. What I see in the future is that a raised cholesterol/LDL level is going to be fully replaced by the LDL/HDL (good/bad cholesterol) ratio as the most important risk factor for CHD. I also see pharmaceutical companies developing drugs that improve the LDL/HDL ratio. Karl Popper in ‘The Poverty of Historicism’ would say that you cannot predict the future by analyzing the past, there are too many variables that you don’t understand. But I believe I can make fully accurate prediction in this area. Any my prediction is this. In five to ten years time, the entire cardiology community will have swept a raised cholesterol/LDL under the carpet, and will look at you with barely concealed amazement if you even dare to mention it as a risk factor for heart disease. We are just entering a Brave New World of risk factor management. Let us do away with lowering LDL, and herald in normalization of dyslipidamia, or ApoA/ApoA(1) ratios. ‘The king is dead, long live the king.’ You think not? Then print this article off, keep it in a drawer and read it again in ten years. You will find that everything I have written has come to pass, exactly as I have predicted. For, when you hear a dog failing to bark, it tells you almost everything you need to know about what is actually going on.
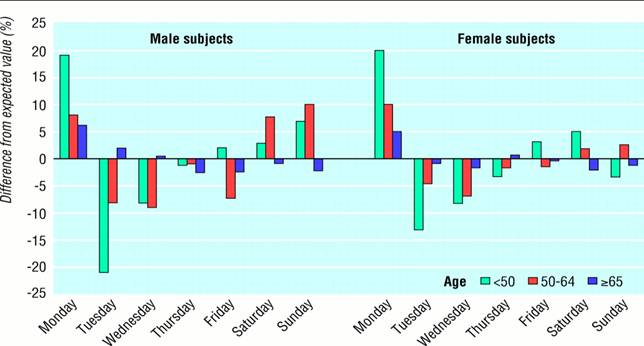
News Item A New And Well-Publicized Study Suggests That Stress Seems To Play A More Important Role In Heart Disease Than Previously Recognized What A Marvelous And Novel Revelation! And Just When Someone Was Trying To Tell Me That Stress, Psychological Or Physical, Has Nothing Whatsoever To Do With Dying Of Coronary Artery Disease By Red Flags Columnist, Dr. Malcolm Kendrick (email - malcolm@llp.org.uk) Here are a few other examples to remind us that memory lapses in science may be more common that we may think.... RESULTS: On days when the local professional football team lost at home, mortality attributable to acute myocardial infarction and stroke increased significantly in men. No increase was observed in women. CONCLUSIONS: Results achieved by the local professional football team are associated systematically with circulatory disease death rates over a five year period in men, but not women. ------------ OBJECTIVES: To examine hospital admissions for a range of diagnoses on days surrounding England 's 1998 World Cup football matches. DESIGN: Analysis of hospital admissions obtained from English hospital episode statistics. SETTING: England. PARTICIPANTS: Population aged 15-64 years. MAIN OUTCOME MEASURES : Ratio of number of admissions for acute myocardial infarction, stroke, deliberate self harm, and road traffic injuries on the day of and five days after England's World Cup matches, compared with admissions at the same time in previous and following years and in the month preceding the tournament. RESULTS: Risk of admission for acute myocardial infarction increased by 25% on 30 June 1998 (the day England lost to Argentina in a penalty shoot-out) and the following two days. No excess admissions occurred for other diagnoses or on the days of the other England matches. The effect was the same when only the two days after the match were treated as the exposed condition. Individual analyses of the day of and the two days after the Argentina match showed 55 extra admissions for myocardial infarctions compared with the number expected. CONCLUSION: The increase in admissions suggests that myocardial infarction can be triggered by emotional upset, such as watching your football team lose an important match. ---------------- Deaths from coronary heart disease occurring outside hospital, by day of week, in people with no previous admissions for coronary heart disease, Scotland, 1986-95: percentage difference from expected values ( See graph)
--------- RESULTS: Cardiac mortality in Chinese and Japanese people peaked on the fourth of the month. The peak was particularly large for deaths from chronic heart disease (ratio of observed to expected deaths) and still larger for deaths from chronic heart disease in California. Within this group, inpatients showed a particularly large peak on the fourth day. The peak was not followed by a compensatory drop in number of deaths. White controls, matched on age, sex, marital status, hospital status, location, and cause of death, showed no similar peak in cardiac mortality. CONCLUSIONS: Our findings of excess cardiac mortality on "unlucky" days are consistent with the hypothesis that cardiac mortality increases on psychologically stressful occasions. The results are inconsistent with nine other possible explanations for the findings-for example, the fourth day peak does not seem to occur because of changes in the patient's diet, alcohol intake, exercise, or drug regimens. --------- The duration of increased cardiac mortality after the 1995 Great Hanshin-Awaji earthquake was longer than seen with previous earthquakes. Further analysis to identify the factors affecting cardiac mortality is needed so that we may reduce adverse health effects during the recovery stage following natural disaster. --------- Death certificates in Eastern Massachusetts after six blizzards in 1974--78, including the record blizzard of Feb. 6, 1978, were examined to identify the effect on mortality of these storms. The total number of deaths was significantly higher (8%) in a "blizzard week" than in the preceding and subsequent (control) weeks (114.1 vs. 105.3 deaths per day). Deaths from ischaemic heart-disease which rose significantly by 22% in the blizzard week from 36.7 to 44.6 deaths per day, accounted for 90% of the excess total deaths. The increase was greater in males than in females (30% vs. 12%), and in both sexes there was no difference in the distribution of deaths by age between the blizzard and control weeks. I.H.D. deaths were increased for 8 days after a snowstorm, suggesting that the effect was related to activities such as snow shovelling rather than the storm itself. --------- RESULTS: Mortality increased substantially after the economic crisis in 1998, with life expectancy falling to 58.9 years among men and 71.8 years among women by 2001. Most of these fluctuations were due to changes in mortality from vascular disease and violent deaths (mainly suicides, homicides, unintentional poisoning, and traffic incidents) among young and middle aged adults. Trends were similar in all parts of Russia An extra 2.5-3 million Russian adults died in middle age in the period 1992-2001 than would have been expected based on 1991 mortality. ----------- Perhaps I should stop here.
More essays by Malcolm Kendrick
|